March 2026
Intermediate to advanced
208 pages
6h 28m
English
In the 1970s, as hospitals began digitizing patient records, a new concept emerged at the intersection of computing and clinical reasoning: the clinical decision support system, or CDSS. These early systems (MYCIN, INTERNIST-1, and later DXplain) did not attempt to replace doctors but were meant to assist them by surfacing probable diagnoses.
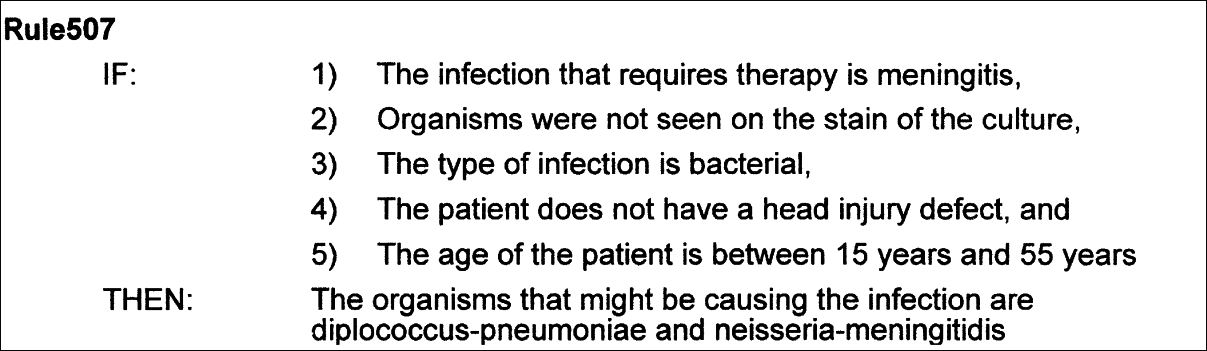
In principle, these systems were intelligent aids, but in practice, they often struggled. One of the reasons was technical: early models couldn’t reason across complex or incomplete patient histories, or evolving treatment protocols. But a deeper issue ran beneath the surface. Even when the logic was sound, the output could be misunderstood. A flagged diagnosis might be taken too seriously—or too lightly. A suggestion might be seen as definitive when it was only probabilistic. Some doctors ignored the systems entirely. Others over-relied on them, treating suggestions as answers. In either case, the interface became the risk surface: the way output was presented and interpreted determined whether it supported or disrupted care. Figure 5-1 shows a standard output from MYCIN, indicating that a bacterial infection may be present if the five conditions in the function are true.
This interpretive problem has become the defining challenge ...
Read now
Unlock full access






